
Donate
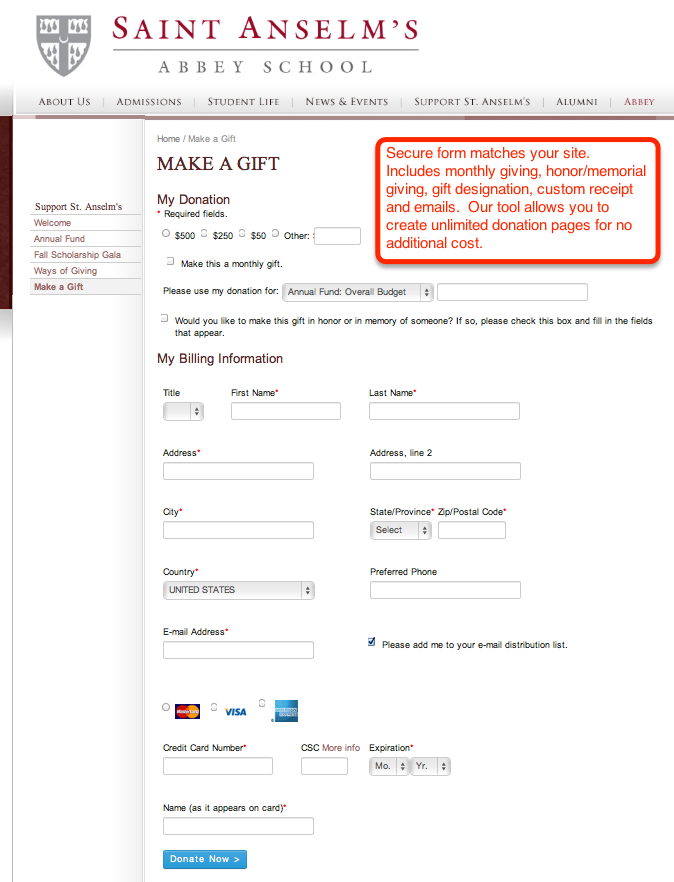
Raise more money with our customizable donation pages, emails, and receipts.
Unlimited campaign pages
Recurring Giving
Honor/memorial gifts with email notifications
Capital campaigns

Most of all I appreciate the personalized and responsive client service that CharityWeb provides - from advice on best practices to quick turn-around on our requests.
Our growth in online donations and registrations has been spectacular!!
All Products: Donate, Register, Peer-to-Peer, Event-A-Thon
30-Day Risk Free Trial
Stripe Merchant Account
Your Look & Feel
Unlimited Pages
Cover the Fee Option
Free Technical Support
Month-to-Month Terms
Monthly Giving
PCI Compliant
Raise more money with our customizable donation pages, emails, and receipts.
Unlimited campaign pages
Recurring Giving
Honor/memorial gifts with email notifications
Capital campaigns

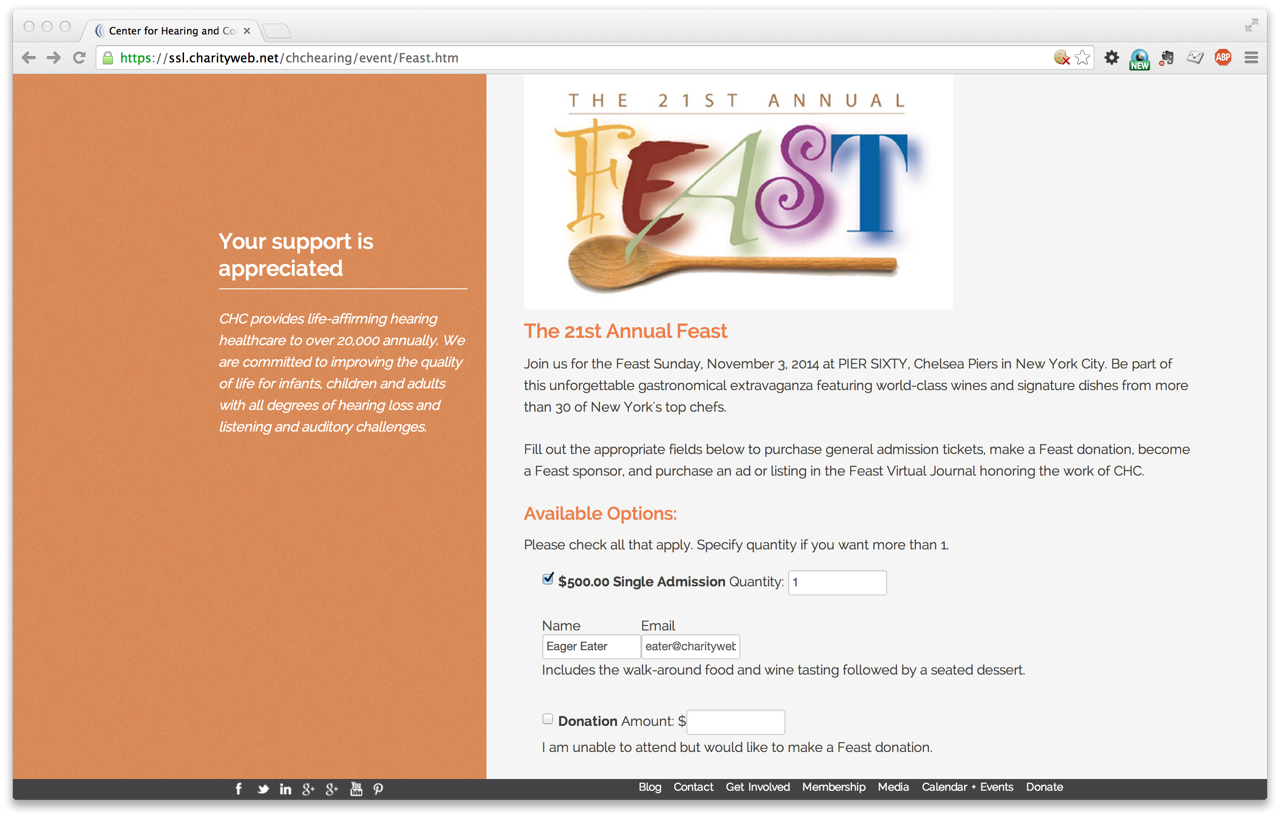
Easily create unlimited registration pages and sell tickets to events with our tool.
Galas
Classes
Golf tournaments
Silent auctions
Gift catalogs

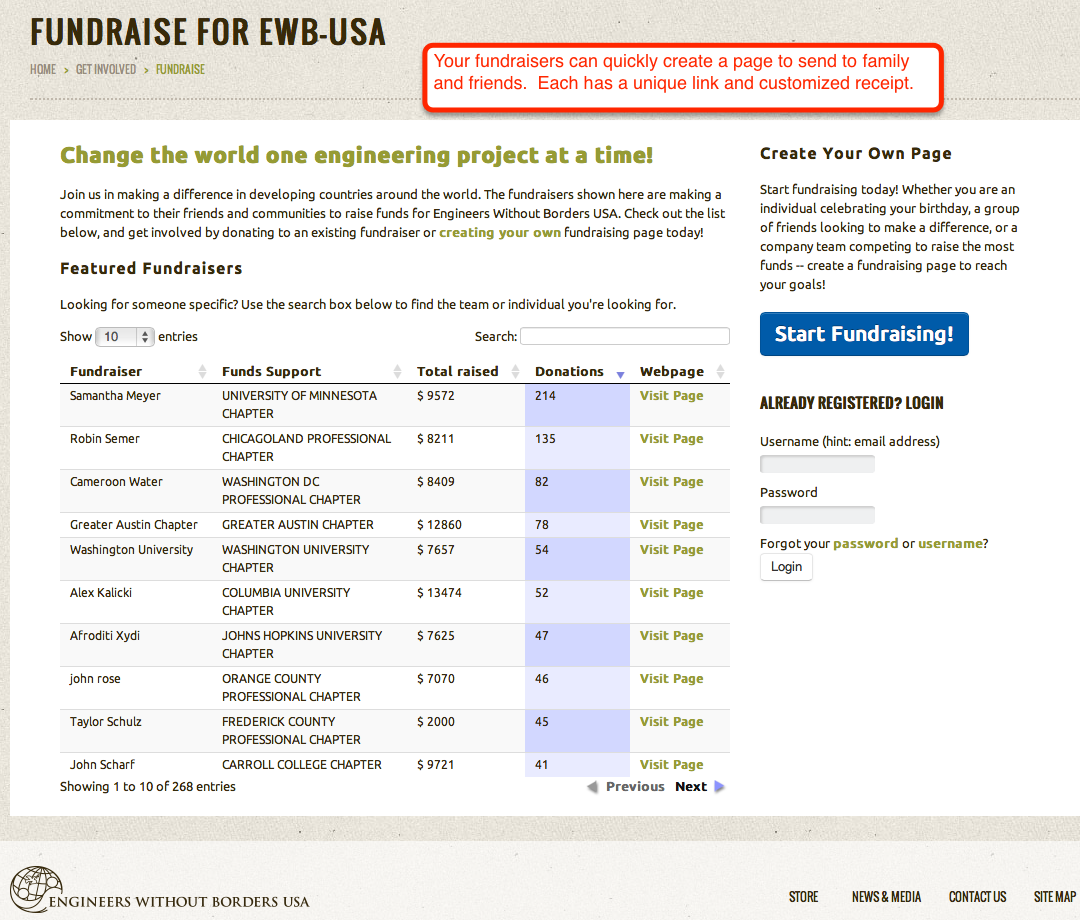
Branded pages give you more control over social fundraising.
Individuals events
Board member campaigns
Alumni campaigns
Giving Tuesday

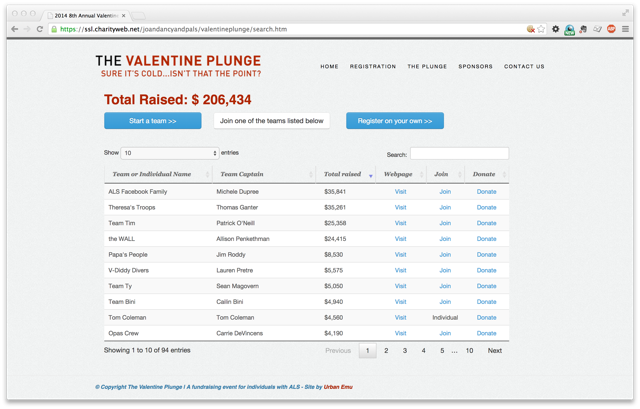
Complete online fundraising system for active, participatory events. Includes registration, team and individual pages, progress bars, leader tables, and customizable emails.
School walk-a-thons
Cold water plunges
Mutt struts
Dragon boat races
*Qualified means 501(c)3. Stripe's standard rate is 2.9% plus 30 cents per transation.
We use Stripe for credit card, debit card, and ACH processing. Stripe charges 2.9% plus 30 cents per transaction initially but drops it to 2.2% plus 30 cents for MC/Visa/Discover and 3.5% for American Express (no 30 cents) once you provide proof of 501(c)3 status.
Getting a Stripe account is quick, easy, online, and integrated with our signup -- you can have a donation page live within a day.
ACH (aka e-check) is available. Stripe fees are 0.8% and are capped at $5 for ACH.
Stripe's fees are simple and transparent. They do not vary depending on the type of affinity card a donor uses. Nor are they loaded up with various other fees you typically see on a merchant account. The 2.2% is not a teaser rate. It is the rate.
We offer the ability for our clients to ask donors to cover the transaction fee by increasing the amount of the donation. Clients can turn this feature on or off on a per donation page basis.
We are unsure how effective this method is at increasing total donations, but it is a feature clients have asked for so we have implemented it.
CharityWeb has been a low cost, high service option for MentorKids USA.
In 1997 online giving was a novelty. Few companies existed to help non-profits raise money online. We set out to change that by creating a company founded on the desire to blend a business opportunity with a chance to do some good. We helped many large charities launch online giving including:
Our clients have raised in excess of $350 Million dollars online using our services, an average of $1.75 Million per client. None of our competitors come close to our per client numbers.
Security and privacy are at the core of our business and are taken very seriously. Click here for our full privacy policy.
We endeavour to act according to the following principles:
Keep in touch with us
{kind=link}
{kind=link}
{kind=link}
{kind=link}